Transfeminine DIY HRT: the Ultimate Guide
Last updated August 2022 • Questions or feedback? Get in contact at hrtinfo@protonmail.com
📝 Contents:
What is HRT?
HRT stands for hormone replacement therapy.
For transfeminine people, this usually means trying to replicate the hormones found in cisgender women.
People
who are assigned male at birth (AMAB) will have higher testosterone levels and lower estradiol (estrogen)
levels
compared to those assigned female at birth (AFAB).
The purpose of HRT is to decrease testosterone levels and raise estradiol levels to levels comparable to
that of
healthy cis females. This is usually accomplished using antiandrogens (blocks testosterone and prevents
masculinization) and estradiol (causes feminization).
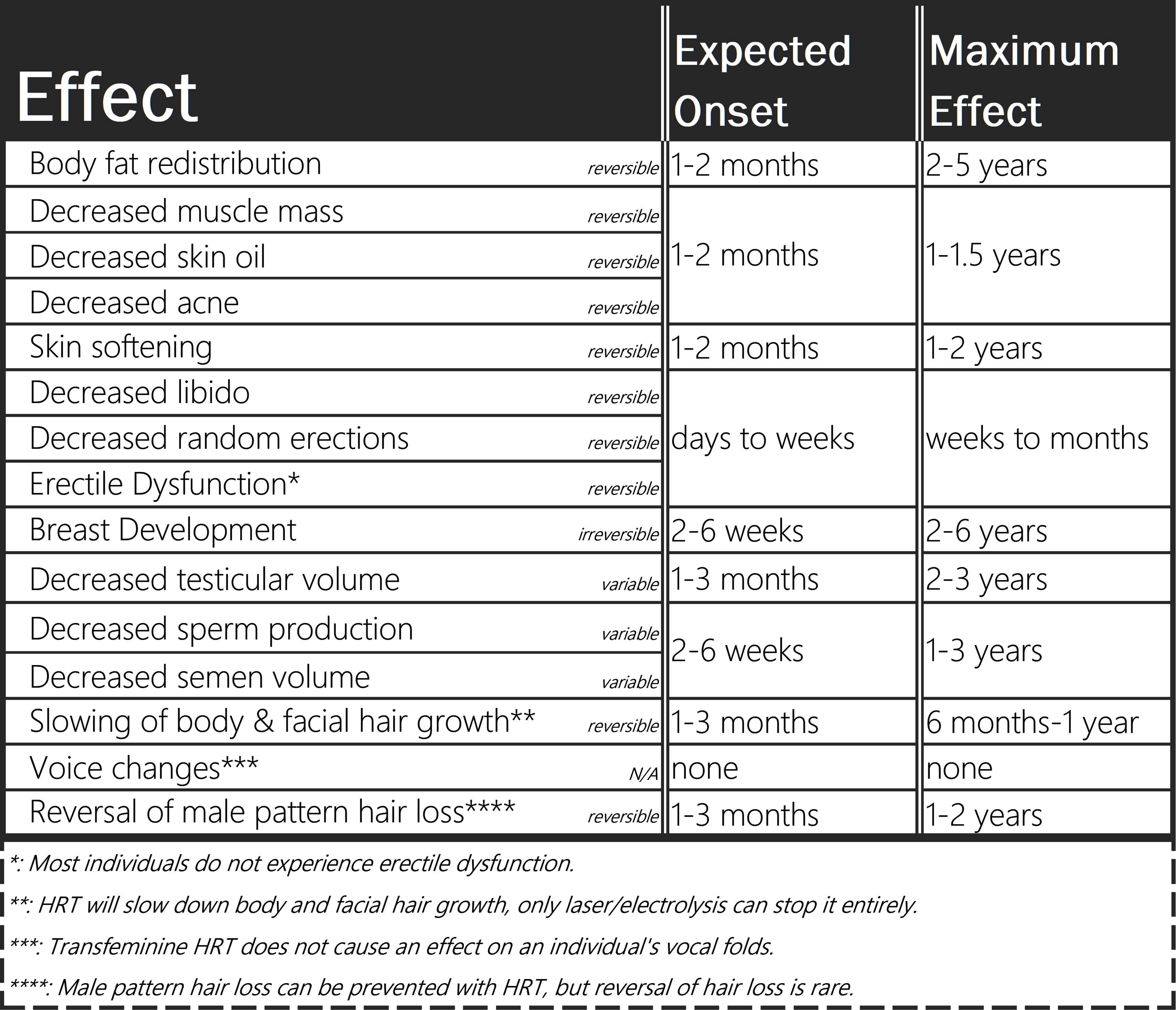
What does it do?
HRT will give a myriad of changes, including breast development, softer skin, fat redistribution more
similar to
that of AFAB bodies and a reduction of libido, among many others.
What methods can I get E in?
There are many forms of HRT and many different kinds of HRT regimens, each with their drawbacks, pros, and
levels of ease in terms of obtaining them.
This section does not cover dosing (see the Dosing section for more information). Given prices
are
rough estimates for DIY sourced HRT.
Prices below are in $USD. Shipping usually goes between $10-35 USD depending on the source. Best to order
at
least several months worth at once to offset the shipping costs.
Pills - $20-$40 per month ($240-480 per year)
By far the most popular and well known, pills are the easiest to come by if you choose to DIY.
Unfortunately,
they tend to be somewhat expensive. Choose bioidentical estrogens (bioidentical means the pills contain the
exact same estrogen produced by human bodies).
Bioidentical estradiol pills usually come in three forms:
Estradiol hemihydrate (e.g. Estrofem, Estrace) is equivalent to estradiol (mostly sold by
homebrewers). Estradiol valerate may also be found in pills. (ex: Progynova) Estradiol valerate has
about
75% of the potency of estradiol or estradiol hemihydrate.
Avoid non bioidentical estrogens such as Premarin or Ethinylestradiol (EE). These carry elevated
thromboembolism (blood clot) risks compared to bioidentical estrogens.
Pills also tend to be quite convenient to take. Also very easy to acquire if you choose to DIY.
Oral intake is simply swallowing your pills. Usually twice per day in ~12 hour intervals. Results in more stable levels versus sublingual/buccal administration.
Sublingual intake refers to placing a tablet under the tongue and letting it dissolve, and buccal intake
refers
to placing a tablet between your gum and the inside of your cheek to dissolve. These two administration
methods
are interchangeable and have essentially the same results.
Sublingual/Buccal administration causes higher peak levels of estradiol in the blood that quickly dissipate.
Because of this, it is recommended that sublingual administration be three (or more) times a day, in 8 hour
intervals.
Transdermal - $30-$45 per month ($360-540 per year)(patches)
Transdermal (estradiol applied to the skin) comes in forms like gels, patches, solutions, etc.
Patches are typically switched out once a week and are designed to give out a set dose of estradiol
every
day. Usually applied to the lower stomach or upper buttocks.
Prescribed gels typically come in packets or in a pump that dispenses a set amount each time.
Estradiol
gels are compounded in an alcohol base to increase absorption. Usually applied to the skin once per day.
Squeeze
tube style gels that aren't properly dosed are not recommended due to difficulty of accurate dosing.
Unfortunately most gels available from DIY sources are in this category.
Solutions are usually sold from homebrewers, containing estradiol in an alcohol-based solution that
is
applied to the skin, usually in an eyedropper style bottle.
Estrogen Creams are not very relevant to transfeminine people because of the low absorption rate into
the
bloodstream and the difficulty of accurate dosing.
Injections - $100-$200 per year
There are certain esters estradiol is commonly compounded in. Estradiol is esterified in order to last
longer in
your body.
Raw estradiol injected into your tissues will very quickly dissipate, which is why estradiol injections all
come
in ester form. It's still just estradiol, your body just slowly converts it into estradiol from its
esterified
form.
Estradiol valerate, estradiol cypionate and estradiol enanthate are the most commonly prescribed and
used
estradiol esters. They all have different half lives (time it lasts inside the body before half the
medication
is metabolized).
Assuming you inject the same amount of estradiol, esters with shorter half lives mean the levels of
estradiol in
your blood and tissues will be higher, but for a shorter period of time.
An ester with a longer half life means you will have to inject a bit more to get to those same peak levels,
but
also means you can inject less frequently.
Estradiol Valerate's (EV) half life is about 3.0 days
Estradiol Cypionate's (EC) half life is about 6.7 days
Estradiol Enanthate's (EEn) half life is about 4.6 days. Although research suggests that the peak of
EEn
comes later than EC. Essentially, treat EEn as similar to EC, with EEn possibly lasting longer.
Valerate is typically prescribed by doctors, with cypionate being occasionally prescribed. Cypionate and
Enanthate are most commonly found sold by homebrewed estrogen sellers.
Pellets - N/A
This cannot be found DIY unless you happen to get it done in a back alley with fake pellets. Don't do that. These are more experimental in terms of dosages compared to the other tried and true methods. You can get them surgically implanted if your insurance covers it. They dissolve E over time and you don't have to worry about missing a dose. They last about 3-6 months. Most doctors that offer pellets compound them to give a patient quite a high dose of estradiol.
Antiandrogens
⚠️ Note:
All of these should be swallowed unless stated otherwise.
Spironolactone (AKA Spiro) - $10-20 per month
Spironolactone is quite a weak antiandrogen, albeit quite safe.
Common side effects include increased thirst, salt cravings and frequent urination.
Can be taken alongside a regular HRT regimen as an experimental erection-prevention drug if getting
erections is
bothersome due to its blood pressure lowering effects (recommend 100-400mg/day¹ for this (start low)).
Not recommended as a first choice of antiandrogen due to its weak anti antiandrogenic effects.
❗ If you are currently taking spironolactone, and your total testosterone (T) levels are under ~30ng/dL,
you
can almost certainly stop taking spiro at that point. The estradiol is doing most of the work of suppressing
your T.
Cyproterone acetate (AKA Cyproterone, Cypro) - $5-20 per month
Cyproterone is a very effective antiandrogen when combined with estrogen.
High doses should be avoided due to a harsher risk profile.
Keeping under a certain dosage is important, especially considering that cyproterone is usually sold in
dosages
4-8 times that of recommended dosages for transfeminine individuals (get a pill cutter!).
Bicalutamide (AKA Bica) - $15-40 per month
Bicalutamide is a very effective antiandrogen, moreso when paired with estrogen. It works in a unique way by
preventing testosterone from having an effect on your body, but it does not actually prevent your body from
producing testosterone. Ironically, this will increase your blood testosterone levels (your body thinks that
you
have zero testosterone inside you and tells your testes to produce even more), but don't worry, all that
extra
testosterone can't do anything.
People tend to report bica being better at preserving penile function, libido and semen volume better versus
other antiandrogens.
Bicalutamide has about a 1/4000 chance of causing either severe liver or severe lung toxicity. It's strongly
recommended to get liver function tests every 3 months if you take bicalutamide.
Estradiol Monotherapy - $100-$200 per year
High enough levels of estradiol in the body is enough to cause your body's testosterone production to lower
significantly. This is usually only easily achievable with estradiol injections, which allow a person to
more
easily achieve high estradiol levels versus other methods of administration.
The vast majority of people on a decent estradiol injection monotherapy regimen (only taking estrogen, no
antiandrogen) are able to suppress testosterone levels adequately without needing to take antiandrogens.
Side Effects/risks:
⚠️ Important Note:
When you google a medication talked about here, you will probably see a massive list of side effects, in the context of antiandrogens, most of these effects (like hot flashes, fatigue, bone density loss, etc.) are actually just side effects of sex hormone deprivation seen in cis men who take antiandrogens without an estrogen for the treatment of prostate cancer. You will not see the effects of sex hormone deprivation if you take estrogen with your antiandrogens.
All recommended tests mentioned in this section can be tested from blood samples taken during a regular blood test. You don't have to get fancy expensive tests.
Estradiol
All forms of estrogens will increase your risk of blood clots (thromboembolism), including serious
blood
clots (e.g. deep vein thrombosis, pulmonary embolism). The likelihood of this is still very low in absolute
risk
but it is present. The risk of getting blood clots on HRT is essentially comparable to that of cis
women
if you take a modest HRT regimen.
Higher levels of estradiol means higher blood clot risk.
Assuming the exact same blood levels of estradiol, taking oral estradiol will carry a higher risk of causing
blood clots versus other forms of administration (due to oral estradiol passing through the liver).
However, because of the higher levels of estradiol in your blood that other methods usually result in
(transdermal, injections, etc.), the unique risks of oral estradiol aren't particularly relevant in
practice.
Spironolactone:
The main reason I recommend against spironolactone is because spiro is a very weak antiandrogen. There are
just
better options out there.
However, it's very safe, but common side effects include increased thirst, salt cravings and frequent
urination
due to it being a diuretic (makes your body get rid of water faster).
Spiro is also known to reduce blood pressure, which can make it hard for some people to attain erections.
Ideally you should get U&E (urea and electrolytes) tested for (see if you're dehydrated, basically) if you
are
on spiro.
Cyproterone acetate:
Extremely high doses of cyproterone, mostly found above 50mg/day and 100mg/day can cause a myriad of
different
harsh side effects and risks, mainly prolactinomas and meningiomas (small benign brain tumors).
At dosages relevant to transfeminine people (6.25-12.5mg/day) the risk profile is much different. The same
risks
are still present but much lower at smaller doses.
Cyproterone is also known to slightly increase blood clot risk, although the increase in risk is quite low
at
dosages used in trans people.
Cypro may increase the risk of B12 deficiency and slightly increase depression risk. Despite the relative
safety
at these doses, ideally you should still get prolactin (PRL) and B12 tested to make sure it's within a
healthy
range. These risks are cumulative (risks gradually get higher the longer you stay on cyproterone).
Bicalutamide:
Due to dysphoria, some transfeminine people do not want to experience a higher libido and an easier time
getting
erections. These are things that bica tends to preserve better than other antiandrogens. Some may see this
as a
beneficial effect, however.
The main risk of bicalutamide is severe liver toxicity and lung toxicity. The chances of either happening
are
about 1/4000. Risk of liver toxicity can be monitored if you get regular liver function tests every 3 months
or
so (done by analyzing blood from a regular blood test sample).
After a year of normal liver function tests, you can stop taking them. The risks of bicalutamide after a
period
of time with no side effects are known to not be cumulative (you can confidently assume that your risk of
lung/liver toxicity will not increase over time if it's already been a period of time without symptoms).
The
risk of both lung and liver toxicity is essentially zero after a year without issues.
Out of the millions of men who have taken bicalutamide for prostate cancer treatment, there have been a few
reported cases where bicalutamide induced a severe light sensitivity condition. Again, the risk for this
does
not seem to be cumulative after a period of time with no symptoms.
Despite these possible side effects, the absolute risk of any severe outcomes occurring on bicalutamide is
extremely low. With the added benefit that bica has essentially no common side effects like spiro or cypro.
GNRH Agonists:
If you have already gone through an AMAB/testosterone puberty, you will experience a temporary flareup of testosterone when you start taking a GNRH agonist for the first time. If you want to avoid this temporary T flare up, you can take cyproterone or bicalutamide for the first 3 weeks of use.
Homebrewed vs Overseas Pharmaceuticals?
“Legit HRT/Pharmaceutical Grade” - Refers to HRT produced by legitimate pharmaceutical
companies
that are licensed and subject to regulation. They are the same quality as those found in your local
pharmacy.
They can be ordered without a prescription from websites based in countries that allow for the legal
exportation
of such medications. These will almost always carry less inherent risk versus homebrewed hormones.
“DIY/Homebrewed” - Refers to HRT produced by individuals, by sourcing raw estradiol
ester/bicalutamide/etc powder and compounding the medication themselves. They do not synthesize (create
from
scratch) hormones. While the concept sounds scary, there are a couple well respected members of the
community
that produce high quality and safe HRT medications.
If you want to acquire DIY injections that aren't prohibitively expensive/difficult to source, homebrewed
injections are the only options available.
Ordering from a homebrewer is usually an easier process due to them being able to speak English well, easier
payment methods, less complicated ordering process and also being a trans person that actually cares about
your
well being.
Blood Testing:
$50-$150 per test, depending on source
Regular blood testing every ~3 months or so is useful, but not absolutely mandatory³, especially if
not
particularly affordable or feasible. Here are some sources of private blood testing⁴ if you cannot access
blood
testing through the medical system:
(USA): https://www.privatemdlabs.com/
(USA): https://labsmd.com/
(USA): https://www.walkinlab.com/
(UK, Ireland): https://www.medichecks.com/
(Canada): https://bloodtestscanada.com/
(Sweden): https://werlabs.se/
(NL): https://www.bloedwaardentest.nl/
(NZ): https://www.pathlab.co.nz/patient-requested/
International sources for blood testing are unfortunately rare. You can try to find local private blood
testing services or ask a doctor if they can provide you with the appropriate blood lab requisition
forms.
Unfortunately, depending on your circumstances, you may be unable to find a way to get blood tests.
Get your estradiol (E2) and total testosterone (T) tested every time. Get your blood taken as close
as
possible to your next scheduled injection/dose (Test your blood as far away as possible from a previous
dose,
right before your next scheduled dose. Preferably the day of your shot, or the day before).
Your blood levels of estradiol and testosterone when taken at this time are called ‘trough levels',
because they are the levels of E2 and T that are present in your body at the lowest point in your HRT dosing
regimen.
Trough levels most useful for injection monotherapy; for determining if your testosterone is
adequately
suppressed at the lowest point of your injection cycle.
The most essential component of transfeminine HRT is to get total testosterone (T) below 50ng/dL and estradiol (E2) above 100pg/mL
For a complete list of recommended blood tests to get, see diyhrt.wiki/bloodtests.
Hormone therapy in general is very safe and effective as long as you take a reasonable dose.
Sourcing/Dosing:
Ideally, you would be on prescribed HRT through legit means. However, you may not have the privilege or
desire,
so this guide may be of use for you.
Regardless, if you are willing to attempt DIY, it is a preferable option to not being on HRT for many.
Prescribed HRT:
If you are in the US: you can try informed consent (Planned Parenthood locations offer this service),
or
any endo that allows it. Informed consent is essentially an easier method of obtaining HRT without having to
prove your transness, or be actually diagnosed with gender dysphoria. You just sign a consent form and
that's
it.
You have to be 18+ to access informed consent services in the USA.
Here is a community-compiled US-centric map that shows clinics offering informed consent:
Erin's Informed Consent Map
. Many new mobile apps and telehealth services in the USA also offer informed consent access to HRT,
see
this short document for a full list for ALL current app/telehealth HRT services: diyhrt.github.io/apps.
To save on prescribed HRT in the USA, try goodrx.com for
free
coupons to use at participating pharmacies. There are no strings attached to this service! Cost Plug Drugs is also a good source
for
affordable medications if you have a doctor's prescription.
If you are in Australia: check to see if your state allows a form similar to informed consent. If you
are
under 16, this may not be available to you. Access to informed consent is variable.
Dr Johnathan Hayes (click here) is an Endocrinologist in St. Leonards that offers
Informed consent.
If you are in the UK: GenderGP (if you can afford it) is a private healthcare service aiding
transgender
people in getting on HRT. It uses a model similar to informed consent and asks about your plan for
transition.
They unfortunately do have a bit of a reputation for giving rather undesirable dosing regimens and can be
quite
expensive.
DIY:
If you do not want to be on waitlists, have to prove your transness while allowing your body to masculinize, or are unable to get HRT legally, DIY may be preferable. Depending on where you order from, you may need to find out how to buy Bitcoin/other cryptocurrencies or find a way to send an international bank transfer, Moneygram, etc. Ordering from a homebrewer may avoid dealing with more frustrating payment methods.
For regimens with antiandrogens:
There is usually no reason to start HRT on a lower than normal dose of antiandrogen, you should go directly
into
a typical dose of antiandrogen and adjust accordingly if needed.
For regimens with oral or sublingual/buccal estradiol:
To accurately dose pills you may need to buy a pill cutter (Amazon or any local pharmacy works). Check your
HRT
source to see if your pills need to be split a certain way for your preferred dosages.
Any regimen:
There's no strong evidence to suggest that starting on a low dose of estradiol and slowly raising your
dose
is necessarily better than starting on a moderate dose. There are anecdotes and theories floating around
that suggest that you may get better breast development or feminization if you start low and slowly ramp
up
your dose. Despite the lack of clinical data and evidence, there's no real harm in doing this. Feel free
to
experiment if you wish.
Antiandrogen + estradiol dosing:
The following example regimens use typical doses of estradiol on the higher end of what would be considered a moderate dose. Adjust accordingly if you have access to blood testing (see blood testing section above).
If you take cyproterone, you will need a pill cutter! (Pill cutters are sold at any pharmacy over
the
counter or online from sites like Amazon). Cyproterone tablets are almost always 25mg-50mg tablets (way over
a
recommended dose). Not recommended to go above 12.5mg of cyproterone daily. Increase estrogen dosage
if
testosterone is not adequately suppressed instead.
Oral estradiol:
Sublingual estradiol:
Estradiol Patches:
Estradiol gel:
Reminder! Bicalutamide causes blood testosterone levels to increase, so even though your T may be adequately blocked, your testosterone levels on a blood test will likely show quite high levels. Bicalutamide also has a long half life, which means it doesn't really matter what time you take it every day, as long as you take it every day. 50mg is almost always enough to ensure adequate testosterone suppression when combined with estradiol.
Oral estradiol:
Sublingual estradiol:
Estradiol Patches:
Estradiol gel:
Buserelin (sometimes sold as the brand name ‘Suprefact') has a short half life, so it should be
administered
three times a day to be effective. You can double the recommended dose of Buserelin during the first week to
counteract the testosterone flare effect that GNRH Agonists have. Alternatively, you can take cyproterone or
bicalutamide for the first three weeks on Buserelin.
Buserelin comes in a bottle that dispenses a set amount of medicine with each spray (300μg per spray in
these
examples).
Oral estradiol:
Sublingual estradiol:
Estradiol Patches:
Estradiol gel:
Monotherapy dosing/Accurate injection dosing:
Here are some reasonable dosages for estradiol injections used in transfeminine hormone therapy:
These dosages should give the vast majority of people high enough estradiol levels to suppress
testosterone
on its own.
Adjust accordingly if you have access to blood testing (see blood testing section above). Ideally you
should
be aiming for the lowest possible estradiol levels (that are still above 100pg/mL) that still adequately
suppress testosterone <50ng/dL at trough. Though people usually require trough estradiol levels of
200-250pg/mL to adequately suppress testosterone.
Vials of estradiol are usually compounded at either 5mg/mL, 10mg/mL, 20mg/mL or 40mg/mL.
This means that for a 40mg/mL vial, every 1mL of liquid will contain 40mg of estradiol. A 40mg/mL 10mL vial
will
then contain a total of 400mg of estradiol.
Homebrewed vials are usually compounded at 40mg/mL.
We will unfortunately be doing some math here.
The formula to calculate how much liquid to inject is: (amount you want to inject) ÷ (concentration of
the
vial) = amount to inject per dose in mL
4 ÷ 40 = 0.1
0.1mL per injection
5 ÷ 40 ≈ 0.13mL
0.13mL per injection
8 ÷ 40 = 0.2
0.2mL per injection
10 ÷ 40 = 0.25
0.25mL per injection
10 ÷ 10 = 1
1mL per injection
10 ÷ 20 = 0.5
0.5mL per injection
Not too complicated now, hopefully!
Cost of needles/syringes - $1-$3 dollars per injection/$50-160 per year (depends on how much you buy
at a
time). Check out our sources for good Injection Supplies
here.
Needles can be bought from any pharmacy over the counter in most countries without a prescription (you may
have
to ask the pharmacist directly).
Most countries also have online sites that sell appropriate injection needles. Amazon is a popular source
for
those in America.
You can also check medical supply sites, which usually have the cheapest prices if buying large quantities.
Make sure to buy 1mL syringes, as the small amounts of fluid we are using for each injection are only
easily measured with 1mL syringes. The more common 3mL syringes will still work if you cannot find 1mL
syringes,
but are not ideal.
There are two methods for an E injection, subcutaneous/subq⁶ (injection into the layer of fat under
the
skin), and intramuscular/IM (injection deep into the muscle underneath the skin and fat). Both
methods
result in identical absorption rates and levels of the drug, whether you prefer subq or IM is mostly
personal
preference.
Homebrewed injections usually hurt less if injected intramuscularly (due to the solvents used in
manufacturing).
Appropriate gauges (needle thickness) for a subcutaneous injection are 25-30g, for intramuscular, 23-25g.
Subq
needles are thinner than IM needles, which some people find less intimidating.
Recommended needle lengths are as follows:
1”-1 ½” (IM, 1 inch is better for thinner people and 1 ½” for thicker people)
½”-⅝” (Subq, up to personal preference)
There are many online videos and guides for how to administer an intramuscular or subcutaneous injection,
here are a few decent ones:
https://getplume.co/patient-resources/
Extremely detailed video guides on both IM and subq injections, with the downside that they are split into multiple long videos. Slightly less professional but shorter guide videos are below:
https://www.youtube.com/watch?v=APSPbpqefKw
https://www.youtube.com/watch?v=W5GAyZzDpNU
Note that around 0.1mL of fluid will be lost with each injection due to needle dead
space.
Be sure to dispose of your needle tips inside of a hard plastic container or a sharps bin to prevent injury!
Sources:
CAUTION: Sources not listed on here or hrt.cafe are risky. Inquire with other members of your community/reddit/etc who ordered DIY from that source before ordering if possible.If you live in a country where companies can legally export HRT medications, that means you can usually
buy
those medications at any local pharmacy without a prescription⁷. The exception would be injections.
Homebrew Sourcing:
Ships domestically ONLY within the UK - Free UK shipping
Accepts cryptocurrency only
Vanna Pharma is a a UK domestic source of homebrewed injections and transdermal estrogen. They have very
good
safety precautions and are a good source to consider if you live within the UK. Unfortunately no
international
shipping. Avoid using their recommended dosages are they are too high for most people.
Ships Internationally from France. Only takes Bitcoin at this time
Sells estradiol enanthate and estradiol valerate vials. Quite a new source. Currently dealing with frequent
stock issues.
International Sourcing (Non-homebrew):
There are simply too many to list, see hrt.cafe for a full list of sources:
Delivery from Russian sites may take longer than other sources (4-8 weeks).
Frequently Asked Questions:
Why do you recommend such low estradiol dosages/levels?
There's no clinical evidence that higher estradiol levels results in better breast development/feminization or a quicker transition. The main factor that determines how quickly breast growth or feminization occurs is adequate suppression of testosterone.
No mention of progesterone (AKA prog)?
Unfortunately, there's a lack of clinical evidence that progesterone has any relevant effects in
transfeminine
people. Despite this, many people have anecdotally reported that progesterone usage resulted in better
breast
development, higher libido, better feminization, mood changes, etc. Progesterone does have potentially
desirable
antiandrogenic effects.
Notwithstanding the lack of evidence for these often-shared anecdotal claims, there are no serious risks of
experimenting with progesterone if you so desire. Of note is that oral progesterone is mostly destroyed by
the
liver. The bioavailability (how much of the medication actually goes into your bloodstream and tissues) of
oral
progesterone is less than 2.4%.
In order for progesterone to be maximally effective, rectal administration is recommended. This
significantly
increases bioavailability of progesterone.
100mg-200mg of rectal prog daily is a typical dose. Most people take rectal prog before bed.
Powers method/Estrone (E1) levels?
Dr. Will Powers is a trans healthcare provider very well known in the trans community. He has made many
claims
about HRT and has a number of unique practices regarding the HRT regimens he prescribes.
There's very little evidence to suggest that Powers' methods are any better at attaining
quicker/better/faster feminization or breast development versus a typical HRT regimen. There is no
clinical evidence that suggests his estrone theory (higher E1 levels during the start of transition with
oral
estradiol causing better breast growth) works any better than other HRT regimens.
The reason Powers' patients tend to get better results is because he prescribes regimens and adjusts levels
based on blood testing so that the patient's hormone levels are actually within reasonable ranges, which is
already quite rare for any trans healthcare provider to do.
Much
of what Powers claims/says are mostly unfounded, and there is much evidence in the contrary for many
of
his claims. This includes his claims about boron, progesterone, the ‘Powers' method', etc.
Despite this, there are some things that Powers has done that are worthy of praise, namely the use of
bicalutamide as an antiandrogen for transfems, using high dose estradiol monotherapy, using rectal
progesterone
instead of oral, etc.
What's the best way of knowing my T levels if I can't get a blood test done?
Content Warning: NSFW mentions of AMAB genitals
There are really no good ways to find out if your T levels are suppressed if you can't access blood tests.
If you ejaculate no or very little semen when you orgasm, it's a likely sign that your T is very adequately
suppressed. However, being able to ejaculate semen doesn't necessarily mean your T isn't being suppressed.
If you notice your libido being significantly higher than normal, an increase in acne/oil production, more
random erections, and increased semen volume, it can be a sign that your testosterone is too high.
Try and avoid relying on very subjective factors like changes in mood to gauge hormone levels.
Do I have to worry about DHT?
DHT is an androgen that causes facial/body hair growth and contributes to male-pattern baldness.
I did not mention DHT in the main guide because:
1) I felt that there would have been too much information in an already info-dense article.
2) HRT regimens that will block/suppress/prevent the effects of testosterone will also do the same for DHT.
Usually it's not something people should worry about.
You can get your DHT tested with a blood test to see if it's too high (I would consider anything >20 ng/dL
to be
high), and add in 0.5mg daily dutasteride (hrt.cafe/dutasteride) to block
DHT.
Is this illegal?
Ordering these medications almost always carries zero risk of legal consequence. This is because in most
countries, estrogens and antiandrogens are not controlled substances that are illegal to order or possess.
However, because ordering medication online without a prescription is unregulated, packages may still be
seized
by customs (essentially the border police that look through mail) and destroyed. Customs seizure is rare
though,
and most sellers will resend a package for free or refund an order if it is seized.
This is how the law works in most countries (including the USA, Canada, UK, EU, most South American
countries,
Australia, etc).
However, ordering from a domestic source (usually homebrew sources) will carry essentially zero risk of
seizure,
because domestic mail does not pass through customs.
Some countries, especially in the Middle East like the UAE, do classify HRT medication as a
controlled
substance.
Research the laws in your country if you are not certain.
↳ What do I do if my package is seized?
In the unlikely event your package is held by customs and you are contacted by phone or email, do not
tell customs what is inside the package.
If they contact you (usually you are only contacted if you provide your contact information to an
overseas
pharmacy source), know that you cannot get in legal trouble for ordering HRT. Contact the seller if
possible
to resolve the issue.
It is bad for people who want to order from a specific seller, and bad for that seller's business if you
tell customs that you're ordering HRT without a prescription. Don't do that.
Traveling with HRT.
Yes it's fine to travel with most HRT. Even with weeks worth of needles and injection supplies. You'll
almost
certainly be fine.
For air travel, be sure your HRT is clearly labeled as what it actually is (write the full name of
the
medication on the bottle/vial/etc if you need to). Don't try to take wrongly labeled HRT onto a plane, for
example, putting HRT pills into a vitamin bottle. If you use injections, store it in your checked baggage.
If you want to be extra safe, throw a bottle of Aspirin and some allergy medication into a large, clear
Ziploc
bag along with your HRT.
Is weight cycling real/worth it?
Content Warning: Food, Weight, Eating Disorders.
Weight cycling is an idea popular in some transfeminine communities. It is the idea that losing weight if
you
are a heavier person pre-HRT, or gaining some weight if you were a skinnier person pre-HRT can help in
obtaining
a more feminine figure/feminine fat distribution and will enhance breast development.
The concept of weight cycling makes intuitive sense, but there has been no research on the subject.
Feel
free to try if you want, just don't hurt yourself or give yourself an eating disorder.
More extreme forms of weight cycling involve repeatedly gaining and losing significant amounts of weight. I
would not recommend this.
Do I have to change my HRT regimen if I get an orchiectomy or bottom surgery/SRS?
If you no longer have testes, you can take a lower dose of estrogen without an antiandrogen, because your body no longer produces significant amounts of testosterone or other androgens, thus negating the need for an antiandrogen. Below are some more tailored HRT regimens for those who have had an orchi or bottom surgery/SRS:
Oral estradiol:
Sublingual estradiol:
Estradiol Patches:
Estradiol gel:
Estradiol valerate
Estradiol cypionate
Estradiol enanthate
📢 References:
¹ For spironolactone, twice a day dosing in 12 hour intervals is recommended (e.g. 50mg twice a day for a total of 100mg per day, or 100mg twice a day for 200mg per day, etc.)
² Supported by evidence in men who take bicalutamide for the treatment of prostate cancer. Bica tends to preserve sex drive better in this population versus other antiandrogens, which can probably be extrapolated to trans populations.
³ However, I strongly recommend regular blood tests (every 3 months) to get liver function tests (LFT) if you are taking bicalutamide, due to the extremely low but still present risk of severe liver toxicity. You can stop these tests after about a year or so (if your liver enzymes are normal on bica after a year you're fine).
⁴ Most private blood testing lets you print off a requisition form, which you can bring to a local blood lab to get your blood drawn. You don't have to mail anything in or take your blood at home.
⁵ If you prefer easier-to-measure amounts, try these alternate dosages:
Estradiol Cypionate (EC): 6mg every 7 days (0.15mL, assuming a 40mg/mL vial)
Estradiol Enanthate (EEn): 8mg every 10 days (0.20mL, assuming a 40mg/mL vial)
⁶ Different abbreviations of subcutaneous in common usage include: subq/subQ, SQ and SC.
⁷ Mexico, China, Brazil, among others.